

Patient 1
This gentleman had diffuse eyelid skin and muscle weakness. In addition to removing redundant eyelid skin and fat, the eyelid muscles had to be strengthened and elevated so that his upper and lower eyelids could return to a more physiological position.


Patient 2
In addition to the redundant eyelid skin and herniated orbital fat that commonly occurs as we age, other aging changes such as growths within the skin may also occur. The yellow plaques seen in this patient are called xanthelasma and are made up of cholesterol.


Patient 3
This patient had both fairly pronounced fat pads as well as a thickened orbicularis or smile muscle.


Patient 4
This patient had weakness in his upper eyelids with resultant visual obstruction and irritation. The eyelid position left him looking fatigued. Blepharoplasty allowed for the sculpting of fat and skin. His eyelid crease was restored allowing for more comfort, better vision, and a more youthful appearance.


Patient 5
This patient had considerable fat prolapse and deep pigmentation of her skin. Blepharoplasty allowed for the removal of prolapsed fat and darkened skin. By removing some overacting muscles in the corners, we were also able to have her upper eyelids open nicely, thereby maximizing her cosmetic result.


Patient 6
This patient has upper eyelid retraction on the right and left brow ptosis. Symmetry was achieved by weakening the right upper eyelid muscle while elevating the left brow. Skin and fat was sculpted from both sides.


Patient 7
This patient underwent an upper and lower eyelid blepharoplasty and tightening of her mid face muscles, along with an endoscopic forehead or brow lift.


Patient 8
This patient had similar surgery but her lower eyelid fat was moved into the hollow areas of her cheeks to prevent a gaunt or hollow post-operative appearance. Note the improvement in the deep furrows all around her eyes.


Patient 9
This patient has ptosis of the right upper eyelid muscle which happened when the nerve to that muscle became disrupted. Surgery involved tightening the upper eyelid muscle.


Patient 10
This patient had her left upper eyelid muscle repaired along with a concomitant blepharoplasty of both upper eyelids.


Patient 11
This patient has mechanical ptosis, which occurs when excessive skin blocks the eye from seeing. Her repair involved the sculpting of skin and redundant eyelid fat.


Patient 12
This patient was an older woman who had skin and fat removed from her upper and lower eyelids; because the underlying muscles were so weak, both the upper and lower eyelids pulled down thereafter. In addition to the haggard appearance, the eyes couldn’t close and were very dry and uncomfortable. Reconstruction involved tightening all of her eyelid muscles and creating a more open and more flattering appearance.


Patient 13
This patient presented with minimal eyelid strength and a very superficial crease. She had multiple folds and the the eyelids were only partially open. She had her eyelids tightened and the crease was made much deeper.


Patient 14
This patient had a very significant amount of eyelid laxity and skin discoloration. He had lost most of the connections that attach the skin to the underlying muscle. He underwent an upper and lower eyelid blepharoplasty as well as a midface lift which supported the muscles allowing for much of that irregular tissue to be excised.


Patient 15
This patient had significant lower eyelid skin redundancy and muscle laxity. Her results were achieved by eliminating the redundant eyelid skin, re-draping the remaining skin to re-adhere to the underlying muscle, then tightening the muscles of the eyelid and mid face.


Patient 16
This patient has pronounced brow ptosis and an almost collapsed eyelid fold. Her brow lift was performed using a combination endoscopic and pre-trichial temporalis lift.


Patient 17
This patient is slightly older and it was felt that endoscopic forehead lifting would not be sufficient to achieve the desired results. A blepharoplasty was performed in addition to her brow lift. Care must always be taken to avoid overcorrection and the inability to have the eyes close properly.

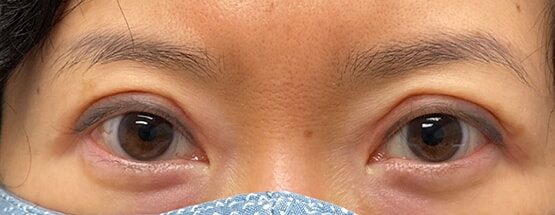
Patient 18
The Asian eyelid is slightly different anatomically than the western eyelid. The septum, which separates the eyesocket from the eyelid tends to be much lower on the eyelid as does the crease. Surgery is geared towards releasing some of the orbital fat and elevating the eyelid crease to a higher position.